A number of radiology practices will not survive the next five years. That’s the conclusion of many industry experts, after analyzing current trends and projected healthcare spending cuts. This white paper presents what the smartest radiology groups are doing today to not only survive, but become more profitable.
Radiology practices are being forced to adhere to a more strict application of the free market—not by their choice, but because the U.S. healthcare market dictates it. In order to attract and retain a qualified pool of radiologists, groups will have to fight off new and aggressive competitive factors, and will be forced to compete with other radiology practices. Accordingly, radiology practices must do everything possible to maintain physician compensation.
Radiologist compensation comes from the profit the business generates. If your group’s revenue is being depleted by the cost of doing business, less money is left for profit or radiologist income. Prior to 2011, groups were able to offset profit loss due to reimbursement cuts with increased productivity and/or smaller practice expense adjustments. That’s not the case anymore.
The Financial Facts
Fixed cost, cost that do not fluctuate with volume of revenue the practice generates, consumes a larger percentage of your income as the gross revenue of the practice declines due to government cuts. And more cuts are coming. This means an increasingly larger portion of your revenue is devoted to costs rather than income. Ideally, costs should move in unison with revenue so, as your revenue declines due to government reimbursement cuts, your costs decline also—maintaining your profit margin.
If internal staff does your billing, that cost is fixed. As a percentage of revenue, internal billing costs increase in a period when revenue is declining. If your billing is provided by a radiology billing company, that cost will vary compared to revenue, because the billing company’s fee is a percentage of revenue collected. Therefore, as a percentage of revenue, outsourced billing cost will decline in a period of declining revenue. Figure 1 illustrates this.
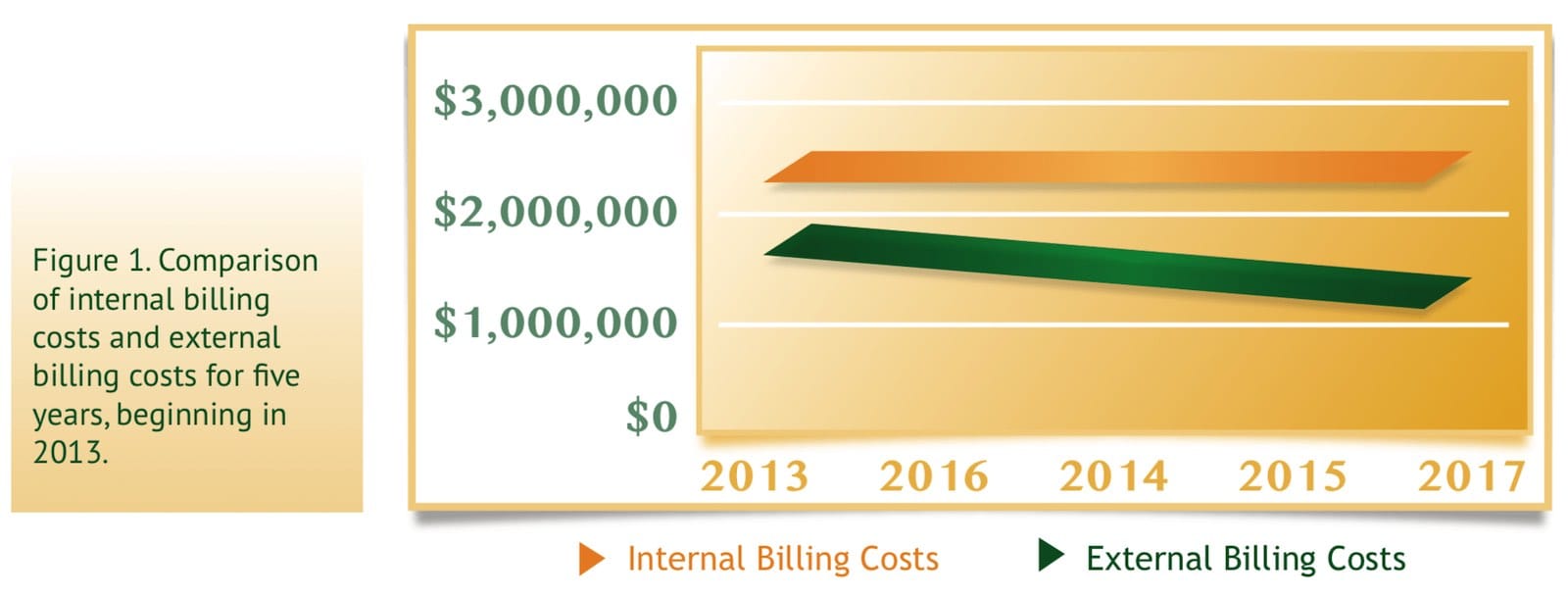
In a period when revenue per exam is increasing, internal billing is more cost- effective. In a period when revenue per exam is decreasing, outsourcing radiology billing is more beneficial. For the foreseeable future, we are working under the latter set of circumstances.
For practices using internal billing, this period of decreasing reimbursement per exam is known as a disruptive event. A disruptive event is a change or increase in the rate of change in an industry; this change or increase creates a new market dynamic and value network, displacing an earlier business process or technology. The term is used in business and technology literature to describe innovations or market forces that change the applicability of a product, service or business function in ways that the market does not expect. In radiology, the disruptive event is making internal billing operations obsolete.
In contrast, a sustaining innovation is one that endows existing markets with better value, allowing the firms within to compete against each other’s sustaining improvements. Sustaining innovations offer a continuous benefit and must be adopted in order to effectively compete in the marketplace. The process of outsourcing to an external radiology specialized-billing company is an example of a sustaining innovation.
In lieu of the SGR, MedPAC recommends an 18% reduction in the conversion factor(CF) for radiology over the next three years,followed by a seven- year freeze in the CF.
Large Reimbursement Cuts are Imminent
Simply stated, without changes, your income will drop by at least 15% over the next five years. Radiologists just can’t increase productivity any further to compensate for this lost revenue. These facts, coupled with severe cuts from the government, create a crucial period for radiologist decision makers. Now is the time for bold leadership in order for your practice to remain viable and more forward.
Specific Medicare Recommendations
The Medicare Payment Advisory Commission (MedPAC) is an independent Congressional agency established by the Balanced Budget Act of 1997 to advise Congress on issues affecting the Medicare program. Historically, MedPAC recommendations have found their way into laws or regulations.
Recently, MedPAC released its “Medicare Payment Policy,” which provides Congress with an assessment of adequacy of current Medicare payment policies and recommendations regarding fee-for-service payments for each healthcare system segment.
The good news is that MedPAC recommends repeal of the sustainable growth rate (SGR) formula. The bad news is that, in lieu of the SGR, MedPAC recommends a 10- year freeze in the Medicare fee schedule conversion factor (CF) for primary care and an 18% reduction in the CF for non-primary care over the next three years, followed by a seven-year freeze in the CF.
MedPAC also gave the following specific conclusions and recommendations to Congress:
- Congress should repeal the SGR system and replace it with a 10-year path of statutory fee-schedule updates. Specifically, MedPAC recommends a 10-year freeze in current CF for primary care services. This would lock in the CF at $33.98 for primary care services. For all other services, MedPAC proposes annual payment reductions of 6% for three years, followed by a seven-year freeze.
- Repeal of scheduled SGR cuts would result in a $300 billion increase in Medicare expenditures over the next 10 years. Freezing the primary care CF and reducing, then freezing, the non-primary care CF would not offset the full cost of repealing the SGR. The repeal/replace approach described by MedPAC would reduce outlays by about $100 billion over 10 years, leaving a $200 billion shortfall to cover an SGR repeal.
- Congress should direct the Secretary to identify overpriced fee-schedule services and bundle codes and/or reduce their relative value units (RVUs), as for CT abdomen and pelvis exams.
- Misvalued Code Initiative: The Patient Protection and Affordable Care Act requires the Centers for Medicare and Medicaid Services (CMS) to periodicall yreview and identify potentially misvalued codes and make appropriate adjustments. The final rule adopts coding changes and value revisions for about 300 services identified as misvalued. CMS identified additional categories of services that may be misvalued, including some of the highest expenditure codes in each specialty not been reviewed during the past five years.
- Congress should increase the Multiple Procedure Payment Reduction (MPPR) to 50%. For calendar year 2012, CMS is applying a 25% MPPR to the professional component (PC) of certain diagnostic imaging services (CT, MRI and ultrasound). CMS claims this new MPPR policy reduces payments for these services by approximately $50 million, which would be redistributed to other services paid under the Medicare Physician Fee Schedule.
In Summary
MedPAC recommendations call for the following over the next five years:
- Drop in Medicare reimbursement by 18%;
- Continued combinations of CPT codes, resulting in decreased reimbursement of more than 10% (2% per year);
- Completion of the RVU reallocation, effectively redistributing radiology income to other specialties, totaling more than 5% (1% per year); and
- An increase in the MPPR to 50%.
The Risk of Not Acting
These very significant industry reimbursement changes are imminent. Many industries have faced similar disruptive events, and every time this occurs, innovative companies display leadership by assessing the business environment and acting accordingly. Companies that ignore such signs of change are doomed for decline or worse. Such obstacles can be overcome.
Today in healthcare, and imaging specifically, ignoring approaching changes and not applying innovations will yield fates similar to those of Kodak, GM and Bethlehem Steel. The risks to inaction are not limited to decreased income.
The risks of not acting also include the following:
- Allowance of additional disruptive events by enabling a whole new competitive force;
- Loss of the entire practice through an exodus of physicians due to noncompetitive compensation;
- Inability to hire new physicians due to noncompetitive compensation;
- Survival by of a forced merger, including loss of identity and decision-making voice; and
- Option of a hospital bailout similar to the fate of 80% of the cardiologists in the United States.
In order for a radiology practice to sustain success and its very existence, the internal and external environment must be analyzed.
Excuses
Good business decisions are based on facts, not emotions. The marketplace has become extremely competitive, containing large, well-run, and well-funded competitors that have your practice in their sights. In order for a radiology practice to sustain success and its very existence, the internal and external environment must be analyzed, and an experienced third-party is best equipped to achieve this and deliver fact-based recommendations to you.
Typically, the reasons given for not outsourcing practice billing include the following:
- We have done it this way for 50 years;
- All billing companies are bad;
- Billing companies are only in it for the money, not for our best interest;
- Our staff has been with us for a long time;
- We are comfortable—why rock the boat; and
- The cost is the same.
How the Math Works
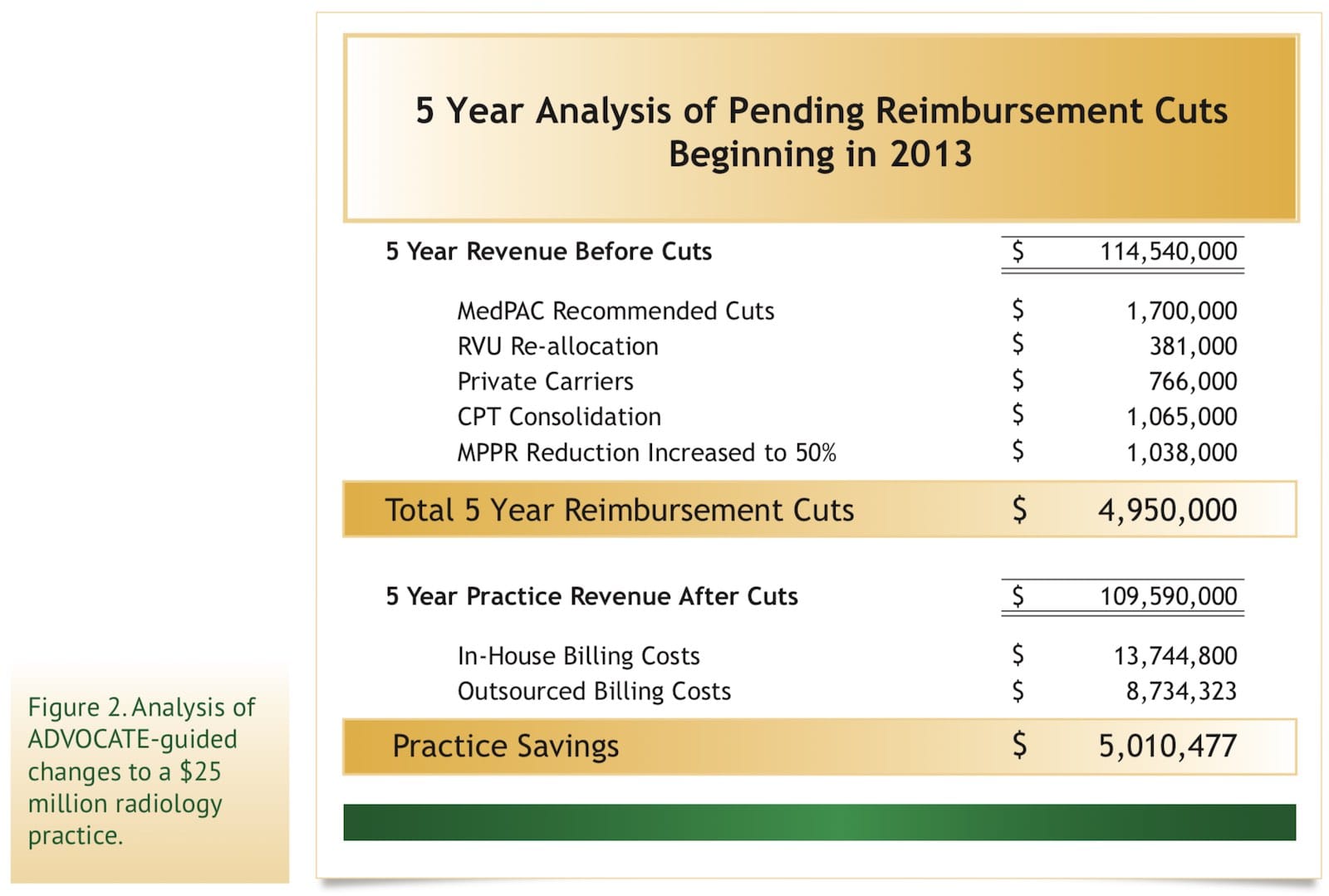
The chart below (Figure 2) illustrates a radiology practice with $25 million in annual revenue. One-hundred percent of the proposed cuts ($4.9 million) are offset by the efficiencies of outsourcing to ADVOCATE, netting the radiologists $5.0 million in additional income over five years. Note: The cuts quantified below include only currently mandated cuts, but more cuts are looming!
The Solution
Not all billing companies are the same. Although billing companies do many of the same things, each has a different history and management style. Just as radiology practices all interpret images, each has a distinct personality and culture.
When considering billing outsourcing and who to select for this partnership, groups should consider the overall outlook for the practice and for the billing company, from multiple angles, over the next three to five years. ADVOCATE’s goal is to help groups identify, evaluate and consider these issues. Our goal is to help you make the right decision by considering the status of where your group is today and where you are headed.
If your group decides to outsource, be aware that many billing companies have a “cookie cutter” process of developing a “one size fits all” approach in which the billing organization focuses attention on their own needs, as opposed to delivering customized service to each client.
Such a cookie-cutter approach results in a rocky transition, culture shock, and insufficient planning, training, and documentation. However, ADVOCATE has developed a proven customized approach, using a dedicated team who specialize in transitioning internal billing operations to ADVOCATE.
Key elements of the customized ADVOCATE transition process include the following:
-
- Maintain existing group strengths;
- Maintain existing group management structure and culture;
- Enhanced reporting and management of the billing process;
- Completely customized approach to each practice; and
- Smooth jointly planned transition components.
</ul
The ADVOCATE Solution – The Transition & Beyond
ADVOCATE’s clients briefly share their success stories:
Tualatin Imaging, P.C., looked at three other outsource-billing vendors before ultimately deciding on Advocate. “ADVOCATE’s director of business development provided an impressive overview of what its outsourced billing service could achieve for us, and I’m pleased to say that Advocate has delivered on all they promised. We could not have experienced a smoother or more professional transition. It’s been an extremely positive experience for the group on all levels.”
—Rae Arendt, Tualatin Healthcare, Tualatin, OR
“We have been completely impressed with ADVOCATE’s responsiveness, professionalism and knowledge of the industry. They have positively impacted every aspect of our practice. ADVOCATE delivered exactly what they promised —a smooth transition and immediate improvements. Going with ADVOCATE was the best decision I made as president of HPRA.”
—Rahul Mehta, M.D., President, HPRA (High Plains Radiological Association), Amarillo, TX
“After considerable review of what improvements needed to be addressed in our billing, service and reporting processes, we found that ADVOCATE provided us with the communication and dedicated billing services to secure the financial support of our practice. We look forward to building a long term relationship with ADVOCATE.”
—James Vasquez, Northern Arizona Radiology
The radiology marketplace is in a period of rapid change that will, likely, drive inefficient practices out of business. It’s a story that has played out in almost every industry. Outsourcing to medical billing experts like ADVOCATE will continue to be a viable option. Groups that do not develop and implement these strategies will be less competitive compared to those that do.
ADVOCATE makes your goal our goal. We educate each prospective and current client, and often end up with a respected friend, as well as a satisfied client. Look for a billing company that will be a leader and business partner. ADVOCATE will structure a customized billing system for you, considering the best transition and results for your group—culturally and financially.